 Français
Français Antibiotic Drugs
Moxifloxacin
Moxifloxacin is a synthetic second generation, broad spectrum bactericidal fluoroquinolone antibiotic.
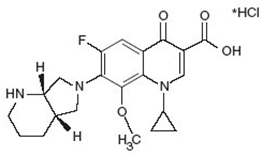
Chemical structure
Its empirical formula is C21H24FN3O4,HCl and MW is 437.9. The chemical structure is:
Mechanism of action
Moxifloxacin inhibits the enzyme bacterial DNA gyrase and prevents replication of bacterial DNA during bacterial growth and reproduction.
Pharmacokinetics
Moxifloxacin is absorbed well when given orally. It has long duration of action allowing once-daily dosing.
Antimicrobial spectrum
Moxifloxacin has enhanced action against gram-positive cocci, mycobacterium tuberculosis, mycoplasma pneumonia, mycobacterium avium complex and anaerobes than ciprofloxacin. It is active against sensitive strains of many gram-positive and gram-negative bacteria.
Indications, administration and dosage
| Condition | Adult dosage/day |
| Acute Bacterial Sinusitis | 400 mg for 10 days |
| Acute Bacterial Exacerbation of Chronic Bronchitis | 400 mg for 5 days |
| Community Acquired Pneumonia | 400 mg for 7-14 days |
| Uncomplicated Skin and Skin Structure Infections (SSSI ) | 400 mg for 7 days |
| Complicated SSSI | 400 mg for 7-21 days |
| Complicated Intra-Abdominal Infections | 400 mg for 5-14 days |
Moxifloxacin is also useful in treatment of multidrug resistant tuberculosis, mycobacterium avium complex in AIDS patients.
Recent trials have shown that moxifloxacin reduces the duration of treatment of drug sensitive tuberculosis.
Precautions, contraindications and warning
Moxifloxacin is contraindicated in patients with known hypersensitivity to moxifloxacin or any other fluoroquinolone. Moxifloxacin should be used cautiously in elderly, pregnancy, nursing mothers, paediatric population and patients with liver or kidney impairment.
Adverse effects
Side effects of moxifloxacin are nausea, diarrhea, vomiting, constipation, abdominal pain, dyspepsia, anemia, fever, headache, dizziness, tendon rupture, photosensitivity, QTc prolongation.
Technical Description on Moxifloxacin
Moxifloxacin is a synthetically derived second generation fluoroquinolone with activity against varied type of bacteria. It is available for both oral and intravenous administration.
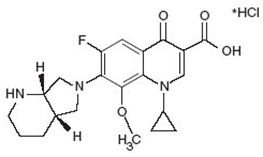
Chemical structure
Its molecular formula is C21H24FN3O4, HCl and MW is 437.9. The chemical structure is:
Preparations available
Oral: 400 mg tablets
Parenteral: 400 mg in IV bag
Mechanism of action
Moxifloxacin like other fluoroquinolones (FQs) causes inhibition of the bacterial DNA gyrase enzyme. This enzyme which causes small cuts in the double-stranded DNA, leads to negative supercoiling and then causes re-ligation of the cut ends. This helps in averting positive supercoiling which may occur in excess. The DNA gyrase comprises of two A and two B subunits: The A subunit leads to small cuts in the DNA, B subunit then brings about negative supercoiling and afterwards the A subunit causes re-ligation. Moxifloxacin attaches to A subunit with great affinity and restricts the above mentioned function of the DNA gyrase enzyme. The predominant target in gram-positive bacteria is an analogous enzyme topoisomerase IV that nicks and separates daughter DNA strands once the DNA replication is complete. The damaged DNA leads to formation of exonucleases resulting in digestion of the DNA and this possibly contributes to the bactericidal action of moxifloxacin.
The cells of mammals have the enzyme topoisomerase II instead of DNA gyrase or topoisomerase IV which possesses very little affinity for moxifloxacin resulting in minimal damage to the host tissue.
Microbiology
Moxifloxacin is active against:
Gram-positive bacteria
- Staphylococcus aureus
- Streptococcus anginosus and constellatus
- Enterococcus faecalis
- Pneumococci
- Streptococcus pyogenes
Gram-negative bacteria
- E. coli
- Haemophilus influenza and parainfluenzae
- Klebsiella pneumoniae
- Proteus mirabilis
- Moraxella catarrhalis
Anaerobic bacteria
- Bacteroides fragilis and thetaiotaomicron
- Peptostreptococcus species
- Clostridium perfringens
Other microorganisms
- Chlamydophila and Mycoplasma pneumoniae
Resistance
Like other fluoroquinolones, resistance is mainly because of chromosomal mutation (Quinolone-Resistance Determining Regions {QRDRs}) forming a DNA gyrase or topoisomerase IV with reduced affinity for moxifloxacin. Another common mechanism is reduced permeability/increased efflux of moxifloxacin across bacterial membranes. Like other FQs moxifloxacin, FQ-resistant mutants are not easily selected hence resistance develops slowly to FQs. However, increasing resistance has been reported among Salmonella, Pseudomonas, staphylococci, gonococci, pneumococci and C. jejuni.
Due to the unique mechanism of action plasmid mediated transferable resistance perhaps does not occur.
A Qnr protein has been seen that offers protection to the DNA gyrase from damage by the FQs. Also modification of moxifloxacin can be caused by a different type acetyltransferase which is similar to the one which modifies aminoglycoside.
Cross resistance is seen within the FQs.
Pharmacokinetics
After oral intake moxifloxacin is absorbed well. Its bioavailability approaches ninety per cent. Moxifloxacin has wide tissue distribution. Plasma protein binding is approximately 40 to 50%. The t1/2 is about twelve hours. It undergoes conjugation with glucuronide and sulfate and then it is eliminated mainly through the kidney and faeces. In animal studies it has been found to be secreted during lactation.
Therapeutic uses and dosage
| Condition | Adult dosage/day |
| Acute infection of the sinuses | 400 mg for ten days |
| Acute Exacerbation of Chronic Bronchitis (bacterial) | 400 mg for five days |
| Community Acquired Pneumonia | 400 mg for 7-14 days |
| Intra-Abdominal bacterial infections (complicated) | 400 mg for 5-14 days |
| Infection of skin and appendages (Uncomplicated) | 400 mg for seven days |
| Infection of skin and appendages (complicated) | 400 mg for 7-21 days |
All the infections mentioned above are caused by the susceptible organism as mentioned in the microbiology section.
Warnings and precautions
- Tendon Rupture and tendinopathy
Like other FQs moxifloxacin can lead to an enhanced chance of inflammation and rupture of the tendons.
- Central Nervous System Effects
Moxifloxacin like other FQs can lead to seizures, increased intracranial pressure tremors, hallucinations, restlessness, anxious behaviour, confusion, depressive state, vivid dreams, and decreased sleep.
- Clostridium difficile-Associated enterocolitis
Clostridium difficile-associated enterocolitis can be seen with moxifloxacin like other antibiotics.
- Peripheral Neuropathy
Rarely large or small sized neurons may be affected by polyneuropathy due to moxifloxacin leading to altered sensations.
- Prolongation of the QT Interval
Moxifloxacin like other FQs can lead to prolongation of the QT interval.
- Phototoxicity
Phototoxic reactions can be seen with moxifloxacin.
- Deterioration of Myasthenia Gravis
Like other FQs, moxifloxacin can lead to deterioration of weakness of muscles in patients of myasthenia gravis.
- Hypersensitive reactions can be seen with moxifloxacin which can be fatal rarely.
- Musculoskeletal Disorders
An increased incidence of musculoskeletal disorders i.e. joint pain and inflammation and Tendinopathy has been observed.
Special populations
- Elderly population
If elderly patients are using steroids there are enhanced chances of tendinopathy in them.
- Children
There are no studies regarding the safety of moxifloxacin in persons aged < 18 years of age. Moxifloxacin has been known to cause arthropathy in young animals.
- Pregnancy
It is a Category C drug. Moxifloxacin was not found to be teratogenic in animal studies.
- Lactation
It is secreted during lactation.
- Kidney dysfunction
Dosage adjustment is not needed in patients with impaired kidney function.
- Liver dysfunction
Liver dysfunction does not affect the pharmacokinetics of moxifloxacin and hence dosage adjustments are not needed.
Contraindications
Moxifloxacin is contraindicated in persons with a history of hypersensitivity to moxifloxacin or any member of the quinolone class of antimicrobial agents.
Carcinogenic potential, Mutagenic and impaired fertility
Animal studies have not shown any concrete proof of carcinogenesis, mutation or impairment of fertility by Moxifloxacin.
Adverse reactions
The following adverse reactions were commonly seen:
- Anemia
- Loose stools, Vomiting, sometimes constipation, pain in the abdomen
- Fever
- Increased levels of Alanine aminotransferase
- Decreased serum potassium levels
- Giddiness, headache
- Decreased sleep
Less commonly seen adverse effects are:
- Decreased platelet count, granulocytopenia
- Hypersensitive reactions