 Français
Français Antibiotic Drugs
Amantadine
Amantadine is a synthetic tricyclic amine of the adamantane family. Amantadine acts as both antiviral and anti-Parkinson drug.
Chemical structure
The chemical formula is C10H17N.HCL and the molecular weight is 187.71.
Mechanism of action- Antiviral
Amantadine inhibits an early step in viral replication.
Antiviral Activity
Amantadine inhibits the replication of each of the subtypes of influenza A virus, i.e., H1N1, H2N2 and H3N2. It has minimal or no activity against influenza B as this virus contains a different protein other than M2 in its membrane.
Mechanism of action- Antiparkinsons
The exact mechanism of action of amantadine in the treatment of Parkinson’s disease and drug induced extrapyramidal reactions is poorly understood. The postulated mechanisms are: - it prevents dopamine (DA) reuptake, facilitates presynaptic DA release, possesses weak antimuscarinic action and blocks glutamate NMDA receptors. It has also been found to antagonize the effects of adenosine at adenosine A2A receptors, which are receptors that may inhibit D2 receptor function. Release of catecholamines from peripheral stores has also been documented.
Action on glutamate NMDA receptors through which the striatal dopaminergic system exerts its influence is now considered to be more important.
Pharmacokinetics
Amantadine is well absorbed after oral administration. Maximum plasma concentrations are directly related to dose. Because amantadine's elimination is vastly dependent on renal function, the elimination t1/2 increases up to 2-fold in the elderly and even more in those with renal impairment. Dose adjustments are advisable in those with mild decrements in renal function.
Indications and uses
Amantadine is indicated for the prophylaxis and treatment of infection caused by numerous strains of influenza A virus.
It is also indicated in the treatment of Parkinsonism and drug-induced extrapyramidal reactions.
| Dose | Duration | |
| Seasonal prophylaxis | 200mg/day | 4-8 weeks |
| Following vaccination during influenza A outbreak | 100 mg/day | 2-4 weeks |
| Uncomplicated respiratory tract illness caused by influenza A virus | 100 mg/day once or twice daily | 5-7 days |
| Uncomplicated influenza A illness | 200 mg/day | 5 days |
| Idiopathic Parkinson’s disease (Paralysis Agitans), post encephalitic Parkinsonism, and symptomatic Parkinsonism | 100 mg twice or thrice daily |
Precautions, contraindications and warnings
The following points should be kept in mind before commencing treatment or prophylaxis with amantadine:
- Amantadine is not a substitute for early vaccination on an annual basis.
- As influenza viruses change greatly over time, emergence of resistance mutations could decrease drug effectiveness. Other factors like changes in viral virulence might also diminish clinical benefit of antiviral drugs. Prescribers should contemplate existing information on influenza drug susceptibility patterns and treatment effects when deciding whether to use Amantadine.
Amantadine should not be discontinued abruptly in patients with Parkinson’s disease since a few patients have experienced a parkinsonian crisis.
Amantadine is contraindicated in patients with known hypersensitivity to amantadine Hydrochloride.
Adverse effects
Most frequent side effects (5-10%) of amantadine are nausea, dizziness and insomnia. Other less frequent (1-5%) side effects include depression, anxiety and irritability, hallucinations, confusion, anorexia, dry mouth, constipation, ataxia, livedo reticularis, peripheral edema, orthostatic hypotension, headache, somnolence, nervousness, dream abnormality, agitation, dry nose, diarrhea and fatigue.
Technical Description on Amantadine
AMANTADINE
Amantadine is a synthetic tricyclic amine of the adamantane family and is designated generically as amantadine hydrochloride. Amantadine is effective as a pharmacological agent in influenza and parkinsonism.
Chemical structure
The chemical name of amantadine hydrochloride is 1-adamantanamine hydrochloride (1-adamantylamine hydrochloride or 1-aminoadamantane hydrochloride).The structure consists of an adamantane backbone that has an amino group (NH2) substituted at one of the four methyne positions. The chemical formula is C10H17N.HCL and the molecular weight is 187.71.
Preparations available
Tablet, capsule - this contains 100 mg amantadine hydrochloride.
Syrup - this contains 50 mg amantadine hydrochloride per 5 ml.
Mechanism of action – as an Antiviral drug
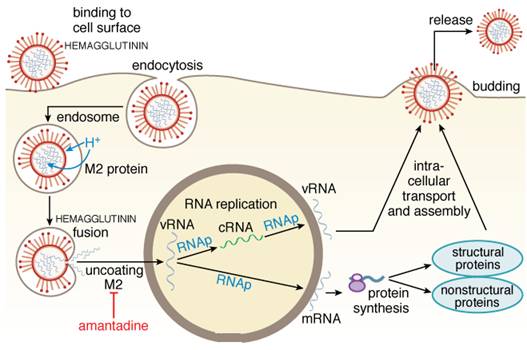
Amantadine inhibits an early step in viral replication, probably uncoating of influenza –A viral RNA within the infected host cells; and for some strains, it also has an effect on a late step in viral assembly possibly mediated through altering hemagglutinin processing. Precisely, the primary target of action is the influenza A virus M2 protein, an essential protein of the membrane which functions as an ion channel. Due to interruption of this function of the M2 protein, the drugs inhibit the acid (H+)-mediated dissociation of the ribonucleoprotein (RNP) complex early in the process of replication. In certain strains of influenza A virus, the pH changes that result from M2 inhibition alter the conformation of hemagglutinin during its intracellular transport later in replication and thus block the viral assembly also.
(See figure below)
Antiviral Activity
Amantadine prevents the multiplication of the following subtypes of influenza A virus - H1N1, H2N2 and H3N2. Amantadine has negligible action against influenza B as this virus contains a different protein other than M2 in its membrane.
Resistance
Resistant variants have been recovered from about 30% of treated children or outpatient adults by the 5th day of therapy and also commonly from immunocompromised patients. Resistant variants appear to be pathogenic and can cause typical disabling influenza. Point mutations results in amino acid substitutions in M2 protein resulting in the rapid development of resistance in up to 50% of treated individuals. The strains which are resistant due to single-point mutations retain their genetic structure and are pathogenic. The use of amantadine has been restricted due to enhanced resistance over the past few years.
Mechanism of Action - as an Anti- Parkinson drug
Though developed as an antiviral drug, amantadine was found serendipitiously to benefit Parkinsonism. The two effects (antiviral and antiparkinson) are probably unrelated. How amantadine acts in Parkinson’s disease is poorly understood. The postulated mechanisms are: - it prevents dopamine (DA) reuptake, facilitates presynaptic DA release, possesses weak antimuscarinic action and blocks glutamate NMDA receptors. It has also been found to antagonize the effects of adenosine at adenosine A2A receptors, which are receptors that may inhibit D2 receptor function. Release of catecholamines from peripheral stores has also been documented. Action on glutamate NMDA receptors through which the striatal dopaminergic system exerts its influence is now considered to be more important.
Pharmacokinetics
After oral intake amantadine is absorbed to a good extent. It is 67% protein-bound. Nasal secretion and salivary levels of amantadine approximate those found in the serum and cerebrospinal fluid levels are 52–96% of those in the serum. Amantadine is excreted in breast milk. Amantadine is eliminated largely without any metabolism through glomerular filtration and probably tubular secretion in the urine. The excretion of amantadine may be affected by the urinary pH. The elimination of amantadine is augmented by acidic urine and by agents acidifying urine. The plasma t1/2 of elimination is ~12-18 hours in young adults. Because amantadine's elimination is vastly dependent on renal function, the elimination t1/2 increases up to 2-fold in the elderly and even more in those with renal impairment. Dose adjustments are advisable in those with mild decrements in renal function.
Indications and usage
- Treatment and prophylaxis of influenza A infection.
- Treatment of Parkinson’s disease
- It can also be used in extrapyramidal reactions induced by various drugs.
Influenza
Seasonal prophylaxis with amantadine (a total of 200 mg/day in one or two divided doses in young adults) is ~70-90% protective against influenza A illness. Seasonal prophylaxis is an alternative in high-risk patients if the influenza vaccine cannot be administered or may be ineffective (i.e., in immunocompromised patients). Prophylaxis should be started as soon as influenza is identified in a community or region and should be continued throughout the period of risk (usually 4-8 weeks) because any protective effects are lost numerous days after termination of therapy. Efficacy has been shown during pandemic influenza, in preventing nosocomial influenza, and in restraining nosocomial outbreaks. Doses of 100 mg/day are better tolerated and still appear to be protective against influenzal illness. Post exposure prophylaxis offers protection of exposed family contacts if ill young children are not concomitantly treated. For the development of antibodies two to four weeks are required after vaccination hence prophylaxis through amantadine should be given for this duration of time. It does not interfere with antibody production.
Upper respiratory tract infections due to influenza A virus particularly uncomplicated are also amenable to treatment by amantadine. But amantadine should be started within first 2 days in such conditions. Treatment is advised in a dose of 100 mg once or twice daily for 5-7 days. Therapy diminishes duration of viral excretion, fever, and other systemic complaints, but resistance has become more widespread with use. Duration of illness is shortened by ~1 day. In uncomplicated influenza A illness of adults, early amantadine treatment (200 mg/day for 5 days) reduces the duration of fever and systemic complaints by 1-2 days, speeds functional recovery, and sometimes decreases the duration of virus shedding.
Treatment with amantadine should be started only after considering the following:
- Vaccination should be given early on a yearly basis and it should not be substituted by amantadine.
- As there is a lot of variation in the influenza viruses over time, resistant strains may develop leading to decreased efficacy of amantadine. Increased virulence may also affect treatment.
Parkinson’s disease
Amantadine is designated for the management of Parkinson’s disease, post encephalitic Parkinsonism, and Parkinsonism caused due to toxic chemicals. Arteriosclerosis of cerebral blood vessels can lead to Parkinson’s disease in elderly population and amantadine can be effective in such patients. Amantadine is not as effective as levodopa in Parkinson’s disease and its benefits may be short-lived, often disappearing after only a few weeks of treatment. Nevertheless, during that time it may favourably influence the bradykinesia, rigidity, and tremor of Parkinsonism. The standard dosage is 100 mg orally two or three times daily. It may also help in reducing iatrogenic dyskinesias in patients with advanced disease. Amantadine is a good drug for patients with mild Parkinson’s disease especially if stated as the first treatment.
Drug-Induced Extrapyramidal Reactions
Extrapyramidal reactions due to various drugs are also an indication for amantadine.
Contraindications
Amantadine is contraindicated in persons with history of prior hypersensitive reactions to amantadine.
Precautions
Sudden withdrawal of amantadine leads to worsening of clinical signs and symptoms in Parkinson’s disease; hence it should not be stopped gradually. Dose of amantadine or anticholinergic drugs have to be adjusted if they are used together and it leads to development of atropinic side effects. Sudden withdrawal can lead to worsening of hallucinations, stupor, delirium, agitation, slurred speech, delusions and anxiety.
In patients taking neuroleptic drugs if the dose of amantadine is decreased or if it is stopped suddenly, it can rarely lead to Neuroleptic Malignant Syndrome (NMS).
Adverse reactions
- Most commonly seen are: Nausea, giddiness, sleep disturbances dizziness
- Less commonly seen adverse effects are: Depression, anxious and irritable behaviour, confusional state, decreased appetite, and dryness of mouth, constipation or sometimes loose stools, livedo reticularis, hallucinations, oedema, orthostatic hypotension, increased sleepiness, nervousness, headache and nasal dryness.
- Least commonly seen adverse effects are: psychotic behaviour, retention of urine, breathlessness, hypertension , heart failure, rashes on the skin, slurring of speech, euphoria, short term memory loss, reduced libido, optic nerve palsy, and abnormalities of cornea
- Rarely seen are: decreased WBC count particularly neutrophils, convulsions, and increased tendency to suicidal attempts.